 August 2006 update
August 2006 update
A collection of research studies compiled by Dr. Martin Dayton to update readers on positive & negative findings in chelation research
August 2006 update
A collection of research studies compiled by Dr. Martin Dayton to update readers on positive & negative findings in chelation research
H. Richard Casdorph, MD, PhD
Dr. Casdorph is Assistant Clinical Professor of Medicine at the University of California Medical School, Irvine California
ABSTRACT: Eight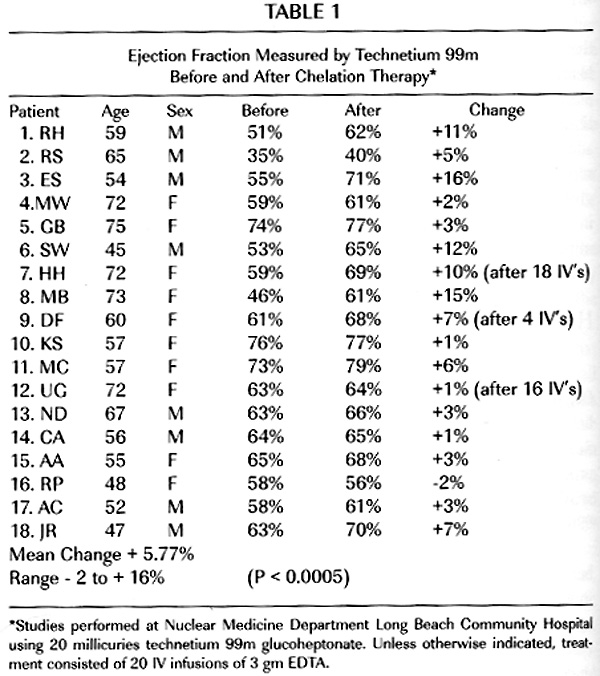 een patients with documented arteriosclerotic heart disease were studied utilizing the radioactive isotope technetium 99m to measure left ventricular ejection fraction before and after the administration of EDTA chelation therapy. A statistically significant improvement in left ventricular ejection fraction occurred in this group of patients. The patients were tested at rest, but conditions under which tests were performed were controlled to be identical before and after chelation.
een patients with documented arteriosclerotic heart disease were studied utilizing the radioactive isotope technetium 99m to measure left ventricular ejection fraction before and after the administration of EDTA chelation therapy. A statistically significant improvement in left ventricular ejection fraction occurred in this group of patients. The patients were tested at rest, but conditions under which tests were performed were controlled to be identical before and after chelation.
http://drcranton.com/chelation/casdor1.htm
 Abstract
AbstractNephropathy is known to occur in persons exposed to high levels of lead, but the question of whether long-term exposure to low levels of environmental lead is associated with impaired renal function remains controversial.
To examine whether chelation therapy slows the progression of renal insufficiency in patients with mildly elevated body lead burden.
Randomized, controlled trial.
Academic medical center in Taiwan.
32 patients with chronic renal insufficiency (serum creatinine level > 132.6 micromol/L [1.5 mg/dL] and < 353.8 micromol/L [4.0 mg/dL]), mildly elevated body lead burden (> 0.72 micromol [150 microg] of lead per 72-hour urine collection and < 2.90 micromol [600 microg] of lead per 72-hour urine collection [EDTA mobilization tests]), and no history of heavy lead exposure.
The treatment group received 2 months of chelation therapy; the control group received no therapy.
The reciprocal of serum creatinine (1/Cr) was used as an index of progressive renal insufficiency.
Rates of progression of renal insufficiency were similar in the treatment group and the control group during a 12-month baseline observation period (1/Cr, 0.000054 L/micromol per month compared with 0.000046 L/micromol per month; P > 0.2). After the 2-month treatment period, improvement in renal function was greater in the treatment group than in the control group. In the 12 months after the treatment period, renal insufficiency progressed more slowly in the treatment group than in the control group (1/Cr, 0.000033 +/- 0.00038 L/micromol per month compared with 0.000045 +/- 0.000038 L/micromol per month; P = 0.0030).
Chelation therapy seems to slow the progression of renal insufficiency in patients with mildly elevated body lead burden. This implies that long-term exposure to low levels of environmental lead may be associated with impaired renal function in patients with chronic renal disease.
Ja-Liang Lin, MD; Huei-Huang Ho, MD; and Chun-Chen Yu, MD
Background: Nephropathy is known to occur in persons exposed to high levels of lead, but the question of whether long-term exposure to low levels of environmental lead is associated with impaired renal function remains controversial.
Objective: To examine whether chelation therapy slows the progression of renal insufficiency in patients with mildly elevated body lead burden.
Design: Randomized, controlled trial.
Setting: Academic medical center in Taiwan.
Patients: 32 patients with chronic renal insufficiency (serum creatinine level > 132.6 µmol/L [1.5 mg/dL] and < 353.8 µmol/L [4.0 mg/dL]), mildly elevated body lead burden (>0.72 µmol [150 µg] of lead per 72-hour urine collection and < 2.90 µmol [600 µg] of lead per 72-hour urine collection [EDTA mobilization tests]), and no history of heavy lead exposure.
Intervention: The treatment group received 2 months of chelation therapy; the control group received no therapy.
Measurements: The reciprocal of serum creatinine (1/Cr) was used as an index of progressive renal insufficiency.
Results: Rates of progression of renal insufficiency were similar in the treatment group and the control group during a 12-month baseline observation period (1/Cr, 0.000054 L/µmol per month compared with 0.000046 L/µmol per month; P > 0.2). After the 2-month treatment period, improvement in renal function was greater in the treatment group than in the control group. In the 12 months after the treatment period, renal insufficiency progressed more slowly in the treatment group than in the control group (1/Cr, 0.000033 ± 0. 00038 L/µmol per month compared with 0.000045 ± 0.000038 L/µmol per month; P = 0.0030).
00038 L/µmol per month compared with 0.000045 ± 0.000038 L/µmol per month; P = 0.0030).
Conclusion: Chelation therapy seems to slow the progression of renal insufficiency in patients with mildly elevated body lead burden. This implies that long-term exposure to low levels of environmental lead may be associated with impaired renal function in patients with chronic renal disease.
Full Content Available for Subscribers: http://annals.org/article.aspx?articleid=712437
In this report, we describe the development of renal function impairment in a 33-year-old patient with mesangial IgA nephropathy and a history of recent gout. Increased body lead burden was identified with a positive EDTA mobilization test. The patient was treated with 1 g of edetate disodium calcium weekly for 2 months until normalization of urinary lead excretion. Improvement of renal function and proteinuria were noted. It was even more interesting to find that both immunofluorescence and electron microscopy studies of the second bio psy specimen revealed the loss of previous mesangial immune deposits. Our case demonstrated that lead may be a nonspecifically damaging factor related to the deterioration of renal function in patients with preexisting renal disease. Moreover, the disappearance of mesangial immune deposits after chelation therapy has not been previously documented. The pathogenetic basis of this observation is unknown, and its causal relationship with lead requires further elucidation.
psy specimen revealed the loss of previous mesangial immune deposits. Our case demonstrated that lead may be a nonspecifically damaging factor related to the deterioration of renal function in patients with preexisting renal disease. Moreover, the disappearance of mesangial immune deposits after chelation therapy has not been previously documented. The pathogenetic basis of this observation is unknown, and its causal relationship with lead requires further elucidation.
 On Feb 23, 2015, the American Board of Clinical Metal Toxicology was dissolved, with its assets given to ICIM. Given our 32 year history educating physicians and championing research on the benefits of chelation and eliminating heavy metals, they deemed it appropriate to pass on the ABCMT legacy. Now ICIM is the trusted steward of maintaining and advancing ABCMT mission.
On Feb 23, 2015, the American Board of Clinical Metal Toxicology was dissolved, with its assets given to ICIM. Given our 32 year history educating physicians and championing research on the benefits of chelation and eliminating heavy metals, they deemed it appropriate to pass on the ABCMT legacy. Now ICIM is the trusted steward of maintaining and advancing ABCMT mission.
When ICIM’s Bylaws were written, John Trowbridge MD had the foresight to include the potential for the creation of Professional Sections within our membership, which would focus on a specific specialty. We have now activated a new Professional Section called Chelation & Metal Toxicology. ICIM members who do chelation will automatically be part of this Professional Section and will have listings on the former ABCMT website, as well as their member profile on www.icimed.com. This should double your search-ability and bring even more attention to doctors who do chelation. Everyone in Chelation & Metal Toxicology Professional Section (affectionately called Chelation PS) is invited to get involved with conference calls to plan and implement our training programs and advocacy for chelation. From now on ABCMT members and ICIM members will be part of one organization, and have only one yearly membership payment.
As President of ICIM, it has my honor to welcome all past members of ABCMT to join our team.
-Ron Casselberry MD
 Dr. Crandall Chaucey: Health report on Chelation, August 2014
Dr. Crandall Chaucey: Health report on Chelation, August 2014
“Whether its called homeopathy, natural therapy or complementary treatment, there’s no doubt that alternative medicine is booming. Today, Americans spend more than $34 billion on these techniques, and surveys show that 1 in 3 Americans have tried some type of alternative medicine…”
Click the link above for the full text pdf.
 L. Terry Chappell, MD: Considering the Past and Promise of Chelation Therapy
L. Terry Chappell, MD: Considering the Past and Promise of Chelation Therapy
Interview by Craig Gustafson
ALTERNATIVE THERAPIES, MAY/JUNE 2014 VOL. 20, 3
L. Terry Chappell, MD, is in private practice with Celebration of Health Association in the cities of Bluffton and Toledo, Ohio. He is board-certified in family practice, geriatrics, chelation therapy, pain management, and advanced longevity medicine. As past president of the International College of Integrative Medicine, past president of the American College for Advancement in Medicine, and as a volunteer assistant clinical professor of medicine at Wright State College of Medicine, he has taught chelation therapy and other integrative medicine to students and doctors from around the world. He has published widely on chelation therapy in scientific journals and in popu- lar books. He has served as a consultant for the National Institutes of Health on several occasions. He has devoted his practice to safe, natural techniques to improve function and help the body heal. He has assembled a high-quality nursing staff and recruited naturopath Bob Angus to work as a team to achieve the best results possible for each individual patient. (Altern Ther Health Med. 2014;20(3):56-60.)
Alternative Therapies in Health and Medicine (ATHM): Did you always know you wanted to be doctor? Was there a specific event in your life that pushed you in that direction?
Dr Chappell: No. When I went to college, I thought that would be about the last thing I was going to be. I had an upper-class roommate who convinced me to try a few class- es, and I tried it, liked it, and I found out I could stand the sight of blood so I went ahead.
ATHM: Where did you go to school, and how did your edu- cation affect your perspective on medicine?
Dr Chappell: I went to DePauw University in Greencastle, Indiana, for undergraduate school. It offered a liberal arts education; you get a good education with a wide back- ground. I think that is very helpful when you are a doctor. Then, I went to medical school at the University of Michigan. That is where my parents did some work, and later my
daughter went there. We have got a lot of connections with the University of Michigan.
ATHM: Were there any particular experiences that—or mentors who—influenced your development as a physician during your medical school years?
Dr Chappell: I would say it was more the broad experience. There was a movement in our medical school class to be of service to underprivileged people and I got involved with that. We established a free clinic, and that was a pretty important influence. I also met my wife through that; she was a nurse in that program. Student Health Organization was the name of it.
ATHM: How did you first come across complementary inte- grative medicine?
Dr Chappell: I first came across it through my wife, who was a registered nurse doing graduate work in psychiatric nurs- ing. Her training involved Lamaze natural childbirth, doing things as naturally as possible, and some nutritional support. That was my first real contact with it. I saw what you could do to relieve pain and stress by nondrug methods. I decided to learn about that. After that, my wife and I did some ser- vice in Appalachia. We found that many of the people there were suffering from pain and depression. They were pre- scribed pain pills and antidepressants, and were not getting anywhere. I looked for some alternatives to help them and they responded very well. They were very interested in it and got me excited about the whole process.
ATHM: What types of things did you find to help the people in Appalachia?
Dr Chappell: I started out by learning ear acupuncture as it is practiced in France. I also learned hypnosis and some basic nutritional tests and treatments. It worked out quite well.
L. Terry Chappell, MD: Considering the Past and Promise of Chelation Therapy Interview by Craig Gustafson
CONVERSATIONS
This article is protected by copyright. To share or copy this article, please visit copyright.com. Use ISSN#1078-6791. To subscribe, visit alternative-therapies.com
Conversations With L. Terry Chappell, MD ALTERNATIVE THERAPIES, MAY/JUNE 2014 VOL. 20, 3 57
ATHM: How much nutritional background did you get in medical school?
Dr Chappell: About half an hour. I have always joked that I was fortunate to get only half an hour of nutrition training because I found out later that most of what they taught was wrong—so I did not have as much to forget.
ATHM: How did you incorporate nutritional and preventive medicine into your practice?
Dr Chappell: I first got into nutritional work actually as a secondary concern. It started when one of my patients kept after me and kept after me to learn more about chelation therapy. We were living in Ohio at that time, where my wife is from. He had people who were working for him who were traveling all the way from Ohio to West Virginia to get chelation treatments. He was seeing great results and he really wanted me to get into it. I was pretty skeptical at that time, but I eventually did agree to visit a couple of doctors who were giving it. I was really impressed by the patients’ stories—how much better they were getting with the treatments. I went to the American Institute for Medical Preventives— later called American College for Advancement of Medicine, or ACAM— so I could learn more about this chelation thera- py. ACAM offered a tre- mendous opportunity to learn about nutritional therapy of all kinds. That is when I really got into it. I found it important to be sure about the quality and the availability of nutritional products. I started ordering them and providing them to my patients—who reaped the benefits. It was a really good move. I went to an intensive seminar by Jonathon Wright, MD, and Alan Gaby, MD. They give these seminars every year or two in which they go into great detail about the scientific paces of nutri- tional therapy. It was particularly fun for me to learn from Jonathan Wright because he was a classmate of mine at the University
of Michigan. We had not seen each other for quite a while, so it was really great to get back together with him and learn about the great work that he was doing.
ATHM: What role does chelation play within the spectrum of preventative medicine?
Dr Chappell: The beauty of chelation is that it removes toxic metals, and toxic metals can interfere with normal function- ing of the body and contribute to disease including immune diseases, circulation problems, and degenerative diseases of all kinds. We find that these are very important to look for. If we find toxic metals, we treat with chelation. Over and above that, chelation helps with circulation, and we believe that if you can improve circulation, you can help most diseases.
ATHM: Are those benefits attributed to the action of a particular chelation agent, or are different sub- stances used?
Dr Chappell: Chelation means to grab ahold of metals and take them out of the body. Some of those are normal metals that you have to replace, but there are chelating sub- stances that have a great affinity for toxic metals such as lead, mercury, cadmium, and arsenic. We use different chelating materials depending on what the toxicity is and what the purpose of treat- ment is. For vascular dis- ease, the best evidence is for EDTA. That was prov- en very nicely by the Trial to Assess Chelation Therapy, or TACT, which was finished a couple of years ago.
ATHM: Tell us about TACT.
Dr Chappell: TACT began as a mandate from US Representative Dan Burton of Indianapolis. He held con- gressional hearings about why the National Institutes of Health, or NIH, was not funding research on chelation therapy even though so many smaller studies pointed to its effectiveness. Eventually the NIH agreed to do the research
This article is protected by copyright. To share or copy this article, please visit copyright.com. Use ISSN#1078-6791. To subscribe, visit alternative-therapies.com
Conversations With L. Terry Chappell, MD58 ALTERNATIVE THERAPIES, MAY/JUNE 2014 VOL. 20, 3
and they called for proposals. TACT was a major double-blind RCT of patients who either got chelation or placebo. They also looked at high-dose vitamins versus low-dose vitamins, and patients received these treatments in addition to their treat- ment for vascular disease. Everybody in the study had suffered a heart attack, so everone had known vascular disease. They looked for cardiac events over 3 to 5 years. The cardiac events included death, new heart attacks, strokes, and hospitalization for severe heart problems. The study wound up with 1708 patients from the United States and Canada. It was a very impressive study and it came out with positive results. This is exactly the type of study that is required of medications to get approval by the FDA and to get accepted in medical circles. With chelation, as it has been a controversial therapy for quite a while, there is still some reluctance to accept it—even though there is proof.
ATHM: Did you participate in TACT?
Dr Chappell: Yes. I was one of the people who originally testified in the congressional hearing, and I was also involved with evaluating the different research proposals that came in. Eventually I did become an investigator in the study, and I did treat patients. We had 39 patients in the study. It was a very good experience.
ATHM: Who was the lead author for that?
Dr Chappell: Tony Lamas, MD. Dr Lamas is a research car- diologist on the faculty of Columbia University and associ- ated with the University of Miami in Florida. He has done several major research projects in the field of cardiology. He is very well respected and he made sure that the study was done without significant problems. It was very interesting because it was one of the first studies that NIH has funded which had university medical centers participating in it along with experienced clinicians out in the field. That coop- eration was very positive.
ATHM: You mentioned that chelation has had controversy surrounding its use. Can you describe why?
Dr Chappell: Chelation was first reported for vascular dis- ease in Detroit by Dr Norman Clarke. Initially, there was a fair amount of interest in it from cardiologists in the United States; this was back in the late 1950s. There was one group of cardiologists that did a study on it, and their conclusion— even though their data was positive for chelation—was that it was not any better than existing treatment. Unfortunately, that eliminated the interest in chelation, and conventional research was no longer done for many years after that. In fact, a small group of alternative doctors continued to use the therapy because they saw really good benefits from it. Quite a number of minor studies were done that supported its use. The AMA and some medical groups became quite criti- cal of the therapy. Finally, the AMA demanded a major study
be done in the early 1980s. Of course, the doctors who were doing chelation did not have the resources to do a large double-blind study. They were treating patients who came to them for help and for treatment, not for a study. It was very difficult to get that study going, though there were several attempts to do it. One started at Walter Reed Hospital, a US Army hospital, but that one fizzled during the Iraq War because the physicians who were doing the study were called off to the war and were not able to complete it. There were other universities that tried to do the studies; they just could not get it done for various reasons. During all this time, medical boards and other medical associations issued statements against the therapy. It was controversial, no doubt, but the NIH finally funded the study.
ATHM: If early trials had shown that it was no more effective than the current treatments, wouldn’t there still be some advantage to using it—considering potential side effects of drug therapy—if it were equally effective?
Dr Chappell: Yes. That is a good point and certainly could be the case. However, I will emphasize that in TACT, in order to prove its effectiveness, all the patients in the study got conventional treatment, so the improvement that they showed in TACT was over and above the conventional treat- ment. It was statistically significant that you could decrease cardiac events pretty substantially with chelation therapy during that trial.
ATHM: Can you comment on the findings coming out of TACT that had to do specifically with diabetic cofactors or comorbidity?
Dr Chappell: That was probably the biggest surprise to con- ventional physicians. Back in the 1960s, there was some work that indicated that diabetics did the best of all the patients, but that was just a couple of isolated studies. In TACT, you could separate out the patients who did have diabetes. The improvement of the patients who had both chelation plus high-dose vitamins decreased the subsequent cardiac events for these patients by 51%. That is a huge num- ber over just a 3- to 5-year period—much more than the usual medications and other treatments that are given for diabetes. The researches who are looking at diabetes are very interested in this, and they are looking at possible further research that might examine this in more detail.
ATHM: Efforts have been made to limit heavy metals in homes and workplaces. If that is the case, why should chela- tion be so important in medicine currently?
Dr Chappell: There is a reduction in lead and mercury in the environment, but there is still quite a bit there. In fact, those metals are both in the top 4 or 5 pollutants in the United States. The chemical toxicities occur and they have been linked to many diseases. Even small amounts of lead and
This article is protected by copyright. To share or copy this article, please visit copyright.com. Use ISSN#1078-6791. To subscribe, visit alternative-therapies.com
Conversations With L. Terry Chappell, MD ALTERNATIVE THERAPIES, MAY/JUNE 2014 VOL. 20, 3 59
mercury can be significant in diseases. This has been shown in many research projects published in the last few years. Unfortunately, up until this time, there has not been a lot of research on treating patients with toxic metals. Small amounts of lead are still big factors in the produc- tion of vascular disease. Why there is such reluctance to treat these patients, I have no idea. It sure makes sense that if you have a toxic substance and you can remove it, then it could make a big difference to that patient.
ATHM: Here in Minnesota, when you think of mercury, you think of fish. But the potential for exposure to mercury is quite a bit greater than most people assume. Where are those environmental exposures to mercury coming from?
Dr Chappell: The biggest one—and still controversial—is from amalgam fillings in teeth. It has been documented that if you have amalgam fillings in your mouth, the metals in them are silver and mercury. If you chew, you can vaporize enough of the mercury so that it can be measured—and it can be high, even toxic levels—just after chewing gum. The mercury amalgam issue is a big one. In some countries those types of fillings are outlawed. Other countries have limited them, but there is still that exposure, because there are an awful lot of people who have amalgam fillings in their mouth. There are other places in the environment: One of the biggest is from burning coal for power. If you breathe polluted air containing mercury, then you are going to absorb some of that into your system. Fish is a big factor, too. If you eat a lot of fish, you can develop a toxic level of mercury.
ATHM: The federal government is pushing one other source into our homes through compact fluorescent bulbs and end- ing the manufacture of incandescent light bulbs.
Dr Chappell: Yes, that is a scary one. If you break a light bulb, that can be a dangerous exposure. You really should call a company that deals with toxic exposures to clean it up. If you try to clean that up yourself, you are going to get a big exposure to mercury.
ATHM: There are several other heavy metals that we need to be aware of in our environment, correct?
Dr Chappell: Right. Arsenic is a big one, and third-world countries are particularly high in arsenic. India, especially, has a huge arsenic problem. Aluminum. Others we are just beginning to understand; one of them is gadolinium. Gadolinium is in the dye that they use for MRIs. When we do a challenge test and look for toxic metals, we can tell whether that individual has ever had an MRI in their lifetime because of high gadolinium levels. Gadolinium is a toxic metal. Tin is another very common one that we see, and nickel, too. Cadmium is very toxic, often related to cigarette smoke, but is also airborne in the environment. We find fre-
quently that people with eye problems have lead or cadmium at high levels. Antimony is another one that can be very toxic. That has been shown in cardiomyopathies; they might have very high levels of antimony. We are just in the beginning stages of understanding the effects of all these toxic metals. Each indi- vidual metal is toxic, but 2 or 3 of them together multiplies the effect and that has not been studied. We certainly think it is a good thing to get rid of them as much as we can. Memory problems: Of course, these have been going up astronomically. Lead, aluminum, and mercury can all con- tribute to memory problems and other neurologic diseases. Often times, if we have patients who have these diseas- es—memory problems, neurologic problems of various kinds, sometimes even cancers—we do a challenge test to see if toxic metals are present. We try to improve their immune system and their neurologic function by removing the metals.
ATHM: You have written about testing for toxic metals and that some of the more obvious tests that have been used in the past may not be tremendously effective or may even be misleading. How so?
Dr Chappell: The gold standard for toxic metals is to do a blood test. The problem is that these toxic metals do not stay in the blood very long. If you are working around them every day and worried you are getting a toxic load, this is fine because you will find elevated levels if there has been a recent exposure. In the body, these metals are stored in the bone, in the brain, and in the fat cells. They are not floating around in the blood. The best way to look for toxic metals is to do a challenge test, where you give a chelating substance and then you mea- sure the urine, or sometimes the stool, to see how many toxic metals you pull out over the next few hours. That is the best way to see if there is a toxic load. This can be really impor- tant. For example, if you have lead in the bone, and you have a bone injury or even maybe a bone surgery, like with a joint replacement, you are going to have leakage of the contents of that bone into the rest of the body and you might get a flood of lead that has been stored in that bone. That could cause adverse effects after a fracture or a surgery that could be very significant.
ATHM: Individuals are engaging in some pretty aggressive detoxification procedures, often without practitioners over- seeing their program. Could this lead to a massive release of heavy metal toxins within the body?
Dr Chappell: Possibly, yes. They have not been well studied, to my knowledge, but I would be concerned about that. You also have to be careful that whoever is doing it is knowledge- able about the chemistry of the substances. For example, EDTA is a very safe substance that is found in tiny amounts in cereals in our grocery store. In higher doses it is used as a chelating substance to pull out toxic metals. Fortunately, it
This article is protected by copyright. To share or copy this article, please visit copyright.com. Use ISSN#1078-6791. To subscribe, visit alternative-therapies.com
Conversations With L. Terry Chappell, MD60 ALTERNATIVE THERAPIES, MAY/JUNE 2014 VOL. 20, 3
becomes tightly bound to toxic metals and is excreted quick- ly. Only about 5% of the EDTA is absorbed orally. You are not going to get a very predictable detoxification with the EDTA given by mouth. Another problem with poor absorbtion of oral EDTA is that it might bind with normal metals and prevent their absorption. So you could get malnourished even though you are eating foods containing the normal metals that you need. It can be controversial. It can be difficult. It has potential for doing harm to a patient, if the person who is doing the treat- ment is not knowledgeable.
ATHM: How about a program where the contents of fat cells are flushed rapidly? They’re losing a tremendous amount of weight in a short amount of time and releasing the contents of those fat cells into the bloodstream.
Dr Chappell: I think that would be an important consider- ation, as well. You could possibly get a flood of toxic metals by releasing them from the contents of fat cells.
ATHM: Considering unavoidable environmental exposures, should there be some level of heavy metal detoxification built into your lifestyle?
Dr Chappell: Certainly regular exercise, particularly if you can build up to a sweat; that is a very good way to detoxify, gradu- ally. Another route is through your digestive tract. If you eat high-fiber foods, you might also benefit from detoxification and prevention of absorbing toxicants from your food supply. Generally with chemicals—and there have been many chemi- cals that have been identified that can be toxic to the body—the body has mechanisms to detoxify and handle those chemicals, but sometimes it does not keep up. I find that milk thistle is a good herb that can be used to enhance the detoxification effect.
ATHM: What about trying to support your body’s antioxi- dant system, like precursors for glutathione?
Dr Chappell: Glutathione is a wonderful antioxidant the body needs. It is essential for many bodily functions. N-acetylcysteine, or NAC, is one precursor that can be used, as well as vitamin E and selenium to help with the produc- tion of glutathione. Glutathione by itself is not very well absorbed into the body, so it is hard to get high levels that way, although there has been some research recently saying that if you use a liposomal preparation you can get much better absorption. There are more products being developed all the time to enhance antioxidant effects, and they are important defense mechanisms.
ATHM: You are currently trying to get the word out about a grant program for chelation therapy. Please describe the program and provide the details for applying.
Dr Chappell: In order to get complete acceptance of chela- tion for toxic metals as well as the use of EDTA for vascular disease, there needs to be another study to support TACT, which was just completed and published—although certain parts of it are still being published. There are not many orga- nizations right now that sponsor research in this area. The NIH is the major one that is a potential sponsor. However, in order to get a major contributor to finance a big study, a lot of work needs to be done. That involves preliminary work, study planning, statistical projections, and so forth. The International College of Integrated Medicine, or ICIM, which teaches doctors how to do chelation safely and effectively, decided to put forward money to stimulate that process. The ICIM has sent out a call for proposals for any- body who is interested in doing chelation therapy. ICIM will give a grant of $20 000 for putting together a proposal for a larger grant and study that can replicate the findings of TACT. This announcement has been received with a lot of enthusiasm, and we expect to get innovative proposals of different diseases that we can test that may support TACT. For example, one thing that has been proposed concerns diabetic patients who have been told that they need an amputation. A study could see if EDTA can prevent amputa- tions. There was a smaller study that actually did show that effect in Denmark. The deadline for the grant is May 31, and ICIM would like to receive as many proposals as possible.
ATHM: Where should the proposals be sent, and how?
Dr Chappell: The proposal should be sent to wendy@icimed.com. Any questions could be directed to her as well. She is the executive director of ICIM.
In the 1980’s, chelation therapy demonstrated great success in treating chronic circulatory problems in several nations around the world. 30 years later, chelation therapy remains a controversial practice that is largely misunderstood in the mainstream population.
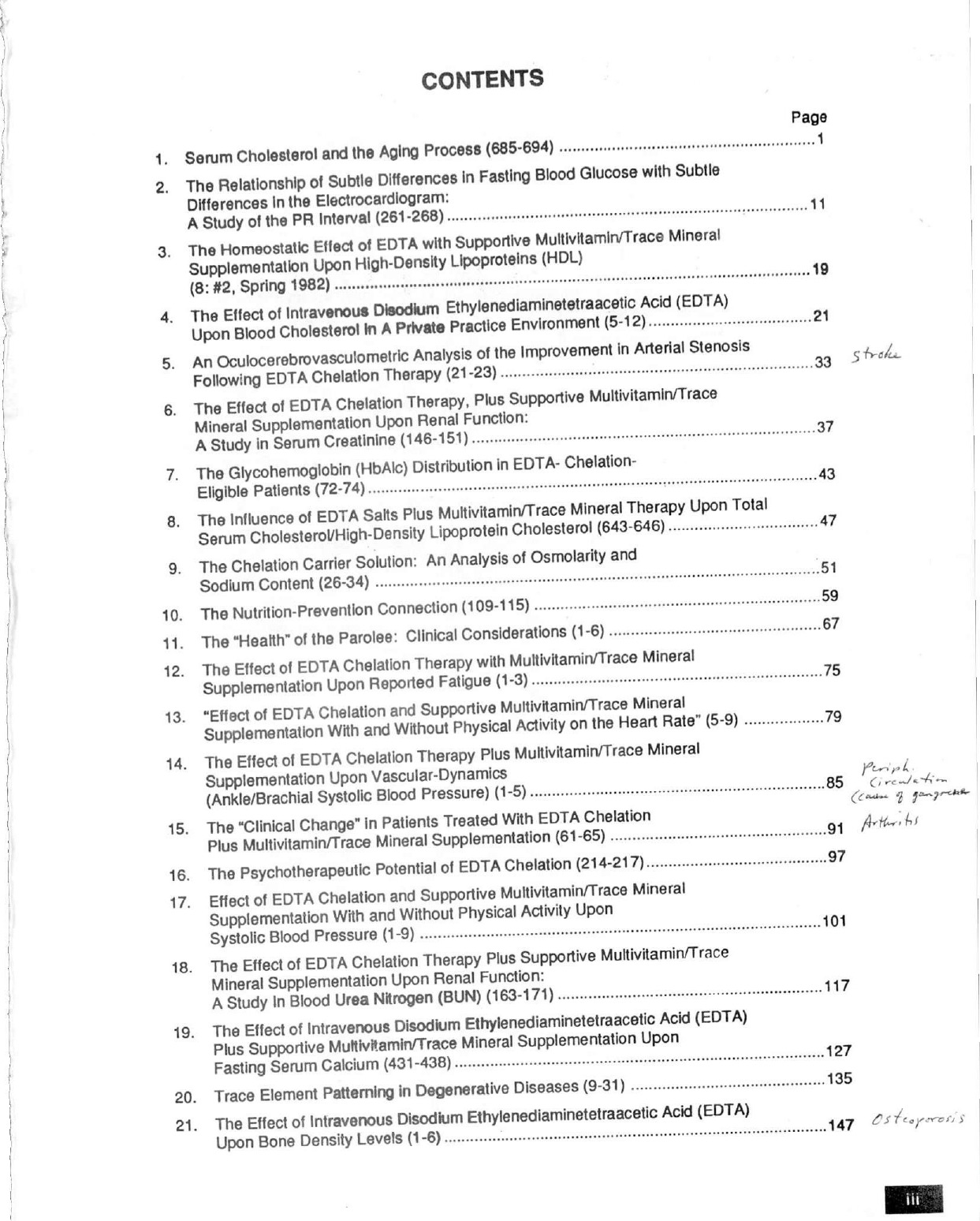
To help inform both the public and other physicians of the benefits of chelation therapy, Edward W. Macdonagh collected research articles containing several studies done globally on chelation. The research was collected and put into a book titled “The Scientific Basis of EDTA Chelation Therapy” which was published in 1981.
Below is the table of contents for the collection of articles by Edward W. Macdonagh and Charles Rudolph DO. Abstracts are available at http://www.mcdonaghmed.com/chelation-therapy/
McDonagh Medical Center Research Articles
 Abstract
Abstract
Intravenous sodium calcium ethylene diamine tetra acetic acid (EDTA) and oral 2,3-dimercaptosuccinic acid (DMSA) have both been used to reduce the burden of lead in humans. Each of these agents enhances the mobilization of lead from different areas of the body – EDTA from the trabecular bone and DMSA from the soft tissue. A study of Korean battery workers revealed that EDTA appeared to increase the soft tissue burden of lead, resulting in increased levels of aminolevulinic acid and greater subsequent lead mobilization with DMSA. This case report discusses a patient with a higher-than-normal lead burden who exhibited increased tissue lead burden after intravenous EDTA. The elevated tissue burden of lead was still present, albeit lower, after five consecutive days of oral DMSA therapy. If this single case is representative of a typical human response to the use of intravenous (IV) EDTA for lead, then it suggests that all persons undergoing such treatment should be administered oral DMSA for a minimum of one week after EDTA treatment.
{kind=link}