Dr L. Terry Chappell, Rakesh Shukla, Jun Yang, René Blaha, Tammy Born, Claus Hancke, William Mitchell, Efrain Olszewer, Peter van der Schaar, James Ventresco;
 23 Aug 2012
23 Aug 2012

Context
Myocardial infarction (MI) and strokes are leading causes of death in the US. Surgical and medical treatments can be helpful, but carry risks of morbidity and mortality.
Objective
To evaluate whether cardiac events were reduced for patients with known vascular disease who were treated with intravenous ethylene diamine tetra-acetic acid (EDTA) chelation therapy.
Design
Retrospective study with a 3-year follow-up, compared with similar patient groups by use of meta-analysis.
Population and setting
A total of 220 consecutive patients with known vascular disease were treated with chelation therapy during 1992–2001. Eight outpatient centres were included: five from the US and one each from Denmark, the Netherlands and Brazil. Average patient age was 64 years, 72.3% were males and 18.2% were smokers. Average number of treatments was 58.
Main outcome measures
MI, stroke and death from any cause were primary outcome measures. Secondary measures were resolution of symptoms and need for coronary artery bypass surgery (CABG) and percutaneous transluminal coronary angioplasty.
Results
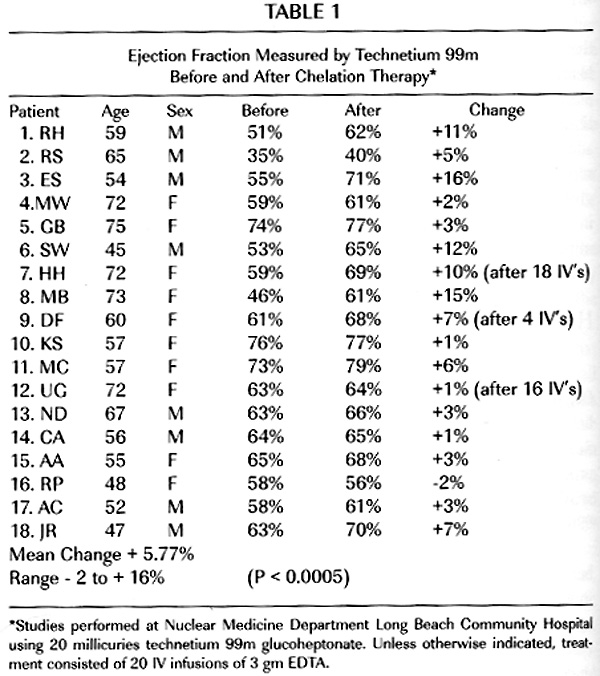
According to the meta-analysis, expected outcomes in a 3-year follow-up period for 220 patients with coronary artery disease treated only with conventional therapies would be 15 MIs and six deaths. There were no deaths and no MIs in this group of patients who received chelation therapy. Four patients had strokes but recovered well. There were two angioplasties and six CABG procedures. Compared with similar patient populations treated with conventional therapies, patients who also were chelated had a 93.6% lesser need for angioplasty and a 62.5% reduced need for CABG. Of the patients that initiated treatment with symptoms, 68.7% had complete resolution of symptoms.
Conclusions
This study indicates that the administration of intravenous EDTA chelation therapy for patients with vascular disease resulted in fewer subsequent cardiac events than primary treatment with CABG, angioplasty or conventional medical therapy. EDTA chelation therapy for vascular disease is a reasonable, off-label adjunct, especially for patients who refuse or are not eligible for surgery. Clinical trials such as the Trial to Assess Chelation Therapy (TACT) are needed for definitive proof.



 50 years, MI
50 years, MI  2.0, assigned to 40 IV chelation or placebo infusions and a 28-component oral MV or placebo. Primary endpoint was death, MI, stroke, coronary revascularization, or hospitalization for angina. Secondary endpoint was cardiovascular mortality, MI, or stroke. We describe the intent-to-treat comparison of 2 factorial groups: chelation + MV (n=421) vs placebo chelation + placebo MV (n=437). Treatment comparisons were by log rank test.
2.0, assigned to 40 IV chelation or placebo infusions and a 28-component oral MV or placebo. Primary endpoint was death, MI, stroke, coronary revascularization, or hospitalization for angina. Secondary endpoint was cardiovascular mortality, MI, or stroke. We describe the intent-to-treat comparison of 2 factorial groups: chelation + MV (n=421) vs placebo chelation + placebo MV (n=437). Treatment comparisons were by log rank test.