Chelation therapy for patients with elevated body lead burden and progressive renal insufficiency. A randomized, controlled trial.
 Abstract
Abstract

BACKGROUND:
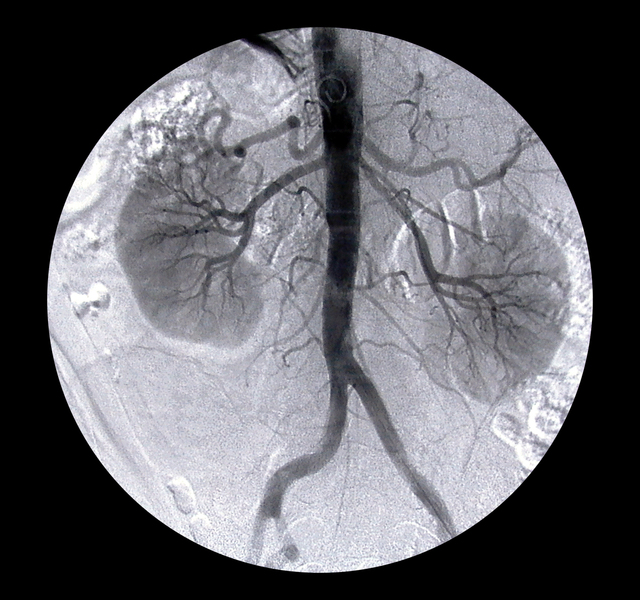
Nephropathy is known to occur in persons exposed to high levels of lead, but the question of whether long-term exposure to low levels of environmental lead is associated with impaired renal function remains controversial.
OBJECTIVE:
To examine whether chelation therapy slows the progression of renal insufficiency in patients with mildly elevated body lead burden.
DESIGN:
Randomized, controlled trial.
SETTING:
Academic medical center in Taiwan.
PATIENTS:
32 patients with chronic renal insufficiency (serum creatinine level > 132.6 micromol/L [1.5 mg/dL] and < 353.8 micromol/L [4.0 mg/dL]), mildly elevated body lead burden (> 0.72 micromol [150 microg] of lead per 72-hour urine collection and < 2.90 micromol [600 microg] of lead per 72-hour urine collection [EDTA mobilization tests]), and no history of heavy lead exposure.
INTERVENTION:
The treatment group received 2 months of chelation therapy; the control group received no therapy.
MEASUREMENTS:
The reciprocal of serum creatinine (1/Cr) was used as an index of progressive renal insufficiency.
RESULTS:
Rates of progression of renal insufficiency were similar in the treatment group and the control group during a 12-month baseline observation period (1/Cr, 0.000054 L/micromol per month compared with 0.000046 L/micromol per month; P > 0.2). After the 2-month treatment period, improvement in renal function was greater in the treatment group than in the control group. In the 12 months after the treatment period, renal insufficiency progressed more slowly in the treatment group than in the control group (1/Cr, 0.000033 +/- 0.00038 L/micromol per month compared with 0.000045 +/- 0.000038 L/micromol per month; P = 0.0030).
CONCLUSION:
Chelation therapy seems to slow the progression of renal insufficiency in patients with mildly elevated body lead burden. This implies that long-term exposure to low levels of environmental lead may be associated with impaired renal function in patients with chronic renal disease.






 . Hg, although for 6 who took autonomic-blocking agents there was a simultaneous reduction of 34 per cent in the requirement for that drug. Of 9 patients who received single doses of 4 Gm. or more of EDTA, 8 quickly developed fever, and in 2 who received large total doses in relation to their body weight, mucocutaneous lesions were observed.
. Hg, although for 6 who took autonomic-blocking agents there was a simultaneous reduction of 34 per cent in the requirement for that drug. Of 9 patients who received single doses of 4 Gm. or more of EDTA, 8 quickly developed fever, and in 2 who received large total doses in relation to their body weight, mucocutaneous lesions were observed.